I wrote this as an assignment for my maternity reflexology training in 2012. My tutor wanted me to publish it. I was a bit too shy to do that but here it is. I see many women with aches and pains associated with pregnancy. Whilst normal in pregnancy, reflexology can help to ease these aches and pains. This article explains how gait and stance is affected by pregnancy and how these changes can affect the pregnant woman.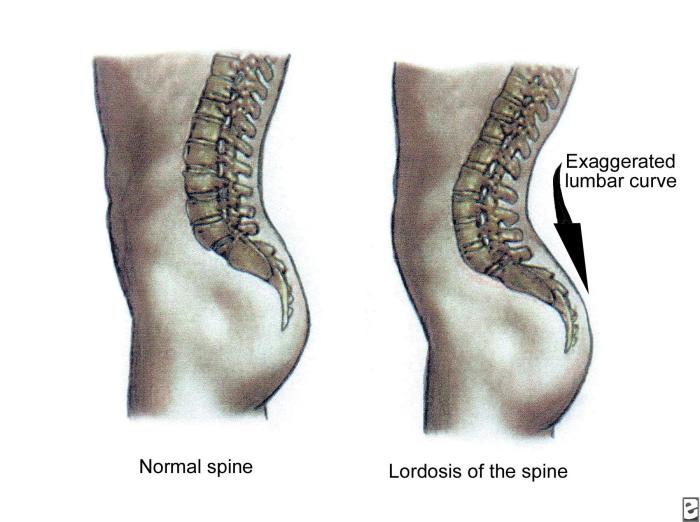
As the photographs above show being pregnant has an impact on the posture or ‘stance’ of the woman. And in turn this effects how she walks or her ‘gait’.
An ideal gait is one where the heel touches the ground first (the foot is ‘supinated’), followed by placement of the whole of the foot on the ground (the foot is ‘pronated’), then the ‘toe off’ (where the foot is ‘re-supinated’ ready for the shift in movement forward again), and then the ‘swing phase’ where the foot swings past the other foot ready to make contact with the ground in front again. Energetically, in an ideal gait, all of the five longitudinal reflex zones are stimulated.
The stance should have pressure on all areas of the foot simultaneously thus again energetically all five longitudinal reflex zones are stimulated.
A study by Hogan et al (2010) found that gait speed, hip angle and pelvic tilt changed during pregnancy. Ankle dorsiflexion also decreased during the gait cycle during pregnancy. As pregnancy develops, women develop an exaggerated lumbar curve (lordosis of the spine) and the pelvis is tilted forward. This stabilises her changing centre of gravity due to the increasing size and weight of the foetus. As the abdominal muscles stretch to accommodate the foetus, proper posture results as the abdominal muscles are less able to contract and keep the lower back in correct alignment.
Also the hormone relaxin is released to soften the connective tissue in the body so the joints are more mobile including the sacral iliac joint. This also includes the ligaments in the foot which can result in the arch flattening (‘over-pronates’).
As the centre of gravity is altered so then the stance changes and how weight is distributed on the foot. The pregnant woman becomes more unsteady on her feet. Riberio et al (2011) found that the pressure on the plantar aspect (sole) of the feet of pregnant women is not different when standing. However, when walking the plantar loads were re-distributed with pressure going from the rear of the foot and increasing to the mid and front of the foot. They concluded that these changes are to help the pregnant woman be more stable during walking.
While Lymbery et al (2005) discovered that there was a wider step width during walking, again to maximise stability and to try to stop the waddling (mediolateral motion) seen often in pregnant women.
A study by Nyska et al (1997) compared the gait of 28 pregnant and 28 non-pregnant women. The change is gait of pregnant women increase the weight bearing on the lateral side of the foot and the hind foot. They went onto conclude that these changes may be responsible for the musculoskeletal complaints of pregnant women.
A reflexologist needs to be aware of the effect that these changes to gait and stance have on a pregnant client. This is because an unsteady gait and unbalanced stance will put the whole body off balance energetically and physically. Extra pressure is put on the hips, ankles and legs. Internal organs that are already out of alignment due to the expanding uterus are even more out of alignment due to pelvic tilt and exaggerated lumbar curve. Due to over-pronation of the foot, the body does not absorb shocks when walking in the usual way. Pressure is put on the foot as weight is transferred from the lateral side of the heel to the medial metatarsus. Not all longitudinal zones are being stimulated as in an ideal gait. The client may not feel very grounded as the whole heel is not striking the ground. The reflexes of the thyroid and lungs are also experiencing more pressure.
In late pregnancy the client is very likely to be suffering from back, hip and pelvic aches and pains as the heaviness of the baby on her ligaments and joints takes it toll. Reflexology can be used to alleviate these aches and pains through the symphysis pubis trigger release, greater sciatic notch trigger release and working well the reflexes of the spine, hips and pelvis.
Late pregnancy can be a time when the reality of giving birth set in and this can make some women feel very scared or anxious. Reflexology can ground and calm the client so that she can feel capable of giving birth. It is likely that the client is not sleeping well and will be feeling tired, uncomfortable and large. Again, reflexology can relax them and tune them into their body, maybe even energising them for a time after the treatment. IF a client already has a child then the reflexology session may give her much needed time out and relaxation.
References
Hagan, L; Wong, C; (2010) Gait in Pregnant Women: Spinal and Lower Extremity Changes From Pre-to Post-partum; Journal of Women’s Health Physical Therapy: May/August 2010 – Volume 34 – Issue 2 – P46-56
Nyska, M, Sofer D, Porat A, Howard C, Levi Meizner I; (1997) Plantar foot pressure in pregnant women; Israel Journal of Medical Sciences: 1997, 33 (2): 139-46
Ribeiro, A, Trombini-Souza, F, Neves Sacco,I, Ruano, R, Zugaib,M, João, S; (2011) Changes in the Plantar Pressure Distribution During Gait Throughout Gestation. Journal of the American Podiatric Medical Association: September 2011, Vol. 101, No. 5, pp. 415-423
Lymbery, J, Gilleard, W: (2005) The Stance Phase of Walking During Late Pregnancy. Journal of the American Podiatric Medical Association: May 2005, Vol. 95, No. 3, pp. 247-253
